A Framework for Reducing Maternal Mortality
Co-created with Ruhani Walia, Navya Riju and Shifra Khan. Special thanks to Stephanie Porfiris, Christina Wang and all of our brilliant advisors for helping make this possible.
I’m working with my other 17-year-old friends to scale misoprostol (a life-saving drug) in Jigawa, Nigeria. We’re developing this system alongside the Jigawa state Ministry of Health, an on-ground team and an advisory network of doctors.
This project aims to reduce the number of deaths due to postpartum hemorrhaging (PPH). PPH is the #1 cause of maternal mortality globally. Maternal mortality kills 300,000+ women every year, and we can save almost ⅓ of them by stopping postpartum hemorrhaging.
While we’re only a few months in, this has been one of the most challenging and expansive experiences I’ve ever had.
This article is part 1 of 2, which goes over the basics of the intervention’s methodology. Part 2 goes over some of our learnings and reflections.
Distribution of Misoprostol to Reduce Postpartum Hemorrhaging in Jigawa, Nigeria
(Don’t worry, the title isn’t as scary or complicated as it sounds.)
Women are dying when they don’t need to. In many countries, there are protocols and health systems in place to give birth safely. But we need global health for humankind, not just for Canada, Finland, Australia, etc.
We have the knowledge, medical protocols and tools to deliver babies safely without injuring the mothers. It just needs to be spread everywhere, specifically to the developing world, where 99% of maternal mortality happens.
Postpartum hemorrhaging (PPH) is the #1 cause of maternal mortality.
PPH is severe bleeding after birth — and it accounts for ~35% maternal deaths worldwide. Some sources say it’s as high as 50% or 60% in some areas.
I won’t go more in-depth into the problem here; you can read more in my blog post on maternal mortality here.
Misoprostol is a uterotonic drug that induces uterine contractions: preventing 85–90% of PPH cases.
Uterotonic = drugs that induce contractions.
Placenta = organ that grows alongside the fetus during pregnancy and needs to be delivered after the baby is delivered. If done improperly, the woman may experience postpartum hemorrhaging.
Using misoprostol after delivery helps induce contractions to remove the placenta safely, preventing 85–90% of PPH cases.
Oral misoprostol is the most ideal uterotonic for low-resource environments.
Oxytocin, ergometrine and syntometrine (which is just the first two combined) are other uterotonics commonly used in developed countries during labour. Oxytocin is the most popular because it is the fastest to induce contractions, and has the fewest side effects (nausea, fever, etc).
All of these drugs require injections/hospital materials and skilled staff to administer them.
Skilled birth attendant rates are very low, with less than 10–20% of births attended by birth attendants in Northwestern Nigeria, where we’re focusing our intervention in. Misoprostol does not require a trained skilled birth attendant or a hospital setting since it is an oral pill. On top of that, it’s >75 times cheaper than oxytocin and >37 times cheaper than ergometrine. In one of the poorest places in Africa, every cent is a barrier.
It is the cheapest uterotonic, and it doesn’t require refrigeration or trained medical staff to administer.
It’s inexpensive, easy to administer, and listed on WHO’s and Nigeria’s essential medicine list.
Especially in rural areas, the facility delivery rate is low, and the traditional birth attendant (TBA) delivery rate is high.
TBAs don’t have formal medical training and many are illiterate. But, the community trusts them more than doctors or health workers. More than half of deliveries worldwide are done by TBAs and over 75% in Nigeria. This number is even higher in rural areas.
In a perfect world, women should deliver in a safe, sterile and highly trained environment. However, systematic change is a long process. If we lean-into the existing infrastructures in these environments, particularly TBAs, we can still save many lives while being cost-efficient.
We are a long time away from a “perfect world.” To increase the feasibility and reduce the friction of change, we want to work with what already exists (TBAs) to distribute what doesn’t (misoprostol).
Why isn’t misoprostol available in rural environments?
Short answer:
- Supply chains don’t extend that far. Most of the supply is located in the cities.
- It’s a stigmatized drug because of its use in abortion pills.
- The community and birth attendants don’t know about its use for PPH. So there’s no demand.
To learn more, I wrote a more detailed article on this topic here.
Nigeria is 2.56% of the world’s population but has 14–20% of maternal mortality cases [1]
Nigeria has the most maternal mortality cases (reported). 5 months ago when we started our analysis we decided to focus our analysis here because of the magnitude of the issue.
We’re doing a Pilot in Jigawa, Nigeria.
Jigawa is a state in North-Western Nigeria with one of the highest maternal mortality ratios (MMR) in the country at 1,012 deaths / 100,000 live births. The 2030 SDG 3.1 goal is to achieve an MMR of 70 deaths / 100,000 live births — we’ll need a ~1,350% reduction in MMR in Jigawa to accomplish this goal. There’s a long way to go, but we need to start somewhere.
Jigawa is 85–90% rural. It has the highest total fertility rate (TFR) in the country at 8.5 children/mother [National Bureau of Statistics].
We chose Jigawa because it met our population criteria to test the intervention (high poverty, rural, high fertility rate, low facility delivery rate, low literacy rate, high MMR).
With data from the Ministry of Health, we started to analyze and select the best local government areas (LGAs) [out of Jigawa’s 27 LGAs] to operate within. These were Jahun, Hadejia and Birnin Kudu LGAs. However, the exact LGA has not been decided yet.
Pilot Goal: distribute oral misoprostol at the cheapest rate possible to save women’s lives from PPH in Jigawa state.
Pilot Outcomes:
- Training 50–100 TBAs. They would reach around 7,200 women, and ~100 will be saved from PPH.
- Collecting data on the mother’s concerns, experience and recommendations for future implementations around the world.
The Intervention Framework has 5 parts:
- Upskilling TBAs
- Supplying the Misoprostol
- Monitoring to Ensure Ethical Usage
- Referrals to Health Centres
- Community Engagement

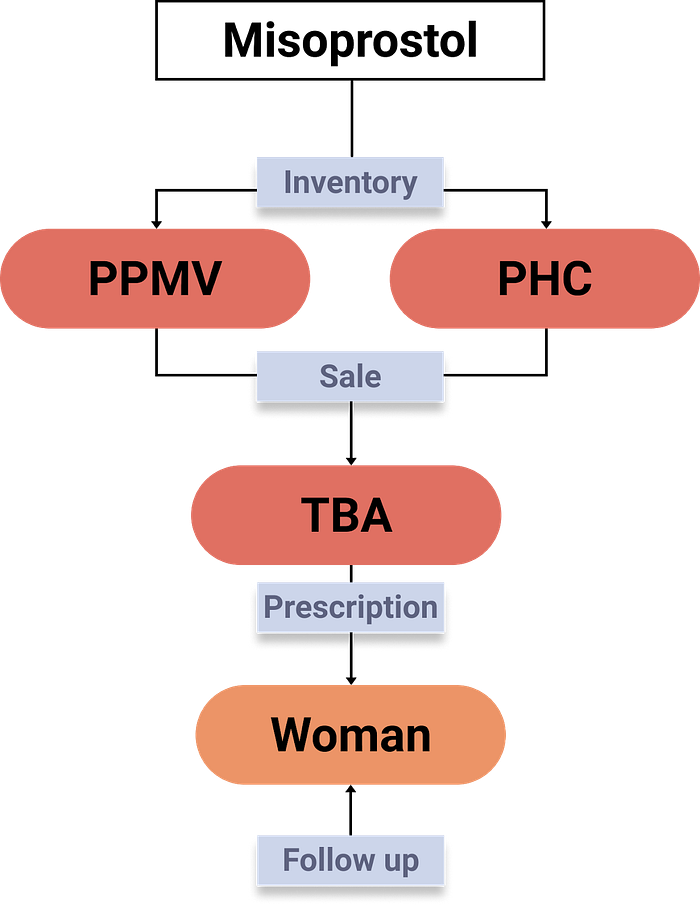
Overall Model
1: Upskilling TBAs
TBAs are trusted by pregnant women, especially in rural areas. They are one of the most optimal pathways to distribute maternal interventions, like misoprostol.
TBAs are less expensive than going to medical facilities and are culturally more trusted by local women. But, the medical community (doctors, midwives, etc.) look down upon their work because they lack medical training. Most TBAs learned through “experience.”
It’s harder to change cultural preferences than it is to train knowledge. TBAs have trust within the community, and we can teach them the medical skills they’ll need to deliver babies safely.
It definitely won’t be easy to upskill illiterate TBAs who are often between the ages of 40–60+. But we have to start somewhere.
We’re focusing the training on the administration of misoprostol for PPH and hospital referrals.
There are 3 steps under upskilling TBAs:
- Designing a curriculum to help TBAs safely administer misoprostol
- Doing a maternal health skill needs assessment among TBAs to inform future training sessions.
- Creating incentives to participate in upskilling
1.1: Designing a PPH curriculum
While there is some information about PPH and safely administering misoprostol, there’s no curriculum designed for TBAs that we could find.
We are trying to train mostly illiterate people. The training needs to be simple, comprehensive and pictorial. The original intent of the training curriculum is for TBAs.
However, technically anyone could participate and learn from the training. If other health workers lacked the knowledge/skills, they could attend a session run using the curriculum.
There are 3 components to the training plan:
- Content (what will be delivered)
- Structure (how we will deliver it)
- Certification (testing their knowledge)
1.1.1: Content:
The training materials focus on PPH treatment in low-resource environments (with the use of misoprostol). Specifically, covering:
- The impact and importance of stopping PPH
- Appropriate dosage and timing
- Side effects
- How to notice adverse effects
- Some knowledge of newborn health protocols (what to do when the baby is born)
We will translate the materials into the local language (Hausa). There are also hand-drawn photos to complement the materials.
Training Package Cover
Special thanks to Christina Wang, David Ye, Farah El Siss and Leah Spalivishi for helping create visuals.
I won’t be publicly sharing the materials because for now. If interested, you can email me (igrandic03@gmail.com) for more details.
1.1.2: Structure:
A 1–2-day workshop delivered in cohorts of 25 trainees.
We’ll start the workshop with a needs assessment evaluation (more on this soon). Then, there are 8 sessions covering different topics. To end off, trainees take another assessment to compare their knowledge before/after the session.
What makes misoprostol great is that it’s simple to use (it’s like taking an Advil). The training materials aren’t that medically dense.
We don’t have a formal timeline for “refresher courses” yet. After a certain period, we’ll want to bring the trainees through a follow-up course to update their knowledge.
1.1.3: Certification:
After the workshop, the final assessment is an assessment of certification. They’ll need to pass this test to become a certified misoprostol provider. There are 20 questions in the test.
There are 3 levels of certification. Our certifications are modelled after the trainer exams from ASHA (India).
Failed: ≤ 12 correct answers
Required to undergo training again.
Passed: 13–16 correct answers
Will have to be tested again after 6 months.
Passed with excellence: ≤ 17 correct answers
Extremely certified to be a misoprostol-administering TBA.
With the certification, trainees will have access to misoprostol procurement centres (more on this soon) at a subsidized rate.
Note: all tests will have the option of being taken verbally in case the trainee is illiterate.
1.2: Needs Assessment
Since we’ll already have several TBAs in a concentrated environment, we can use the opportunity to understand their knowledge gaps in maternal and newborn health. We can use these results to inform future policy/budgeting strategies.
The needs assessment will encompass more testing material than just PPH. But there will still be a PPH-related section in this needs assessment. (We will use the PPH section’s results to compare to the end-test results, to test the effectiveness of the training).
We’re working with doctors to create a general maternal and child health knowledge needs assessment test.
1.3: Incentives
The incentives covered in this section are:
- Starting their own “Misoprostol Business” [profit]
- Village recognition
- Training Attendance Stipends
1.3.1: Starting their own “Misoprostol Business.”
Once trainees are certified, they’ll have access to misoprostol, which they’ll sell to their customers (women) at a regulated price to keep it affordable — more on the selling protocol under the “TBA Storage” section.
Their supply of misoprostol will be a lot cheaper than what they could find elsewhere. This is because we’re purchasing “hospital packs” worth of misoprostol, which are very large (400 pills). We will then sell a minimum of 8 pills, and a maximum of 32 pills to each TBA at the hospital price unit cost. They get a better deal per pill without spending a lot of money upfront and they can make a profit off of the re-sale.
1.3.2: Village Recognition
Communal recognition is essential to TBAs [2]. Specifically, recognition from religious and traditional leaders.
The community trusts TBAs. We can use their trust to save lives. We should recognize that: this may be through gifts, media attention or dinner with leaders.
1.3.3: Training Attendance Stipends
Many health training sessions pay their trainees to attend and, in addition, provide gifts afterwards. I can’t put a dollar to the cost per attendance yet, but here are few incentive expenses we’re considering:
- Branded Hijabs, T-shirts, or other commonly-worn clothing
- Bicycle/Tricycle or other forms of transportation
- Mobile phone (this would double as a data-collection input device)
- Initial starting supply of Misoprostol (or other handy birthing supplies like a clamp or towel).
- Monetary incentive
There are also some expenses with running the training like venue, trainer, food, etc. Depending on the budget and expenses, we will decide the scope for training attendance stipends.
With trained, certified and incentivized TBAs, we can move on to distributing misoprostol.
2: Supplying the Misoprostol
We need misoprostol to be financially and physically accessible within the community.
Financial Accessibility
In a poor, rural population, every cent is a new barrier. The less expensive we can make misoprostol, the better.
We’ve set a target selling price for below 350 Naira (0.91 USD). However, some local feedback has encouraged us to bring the target price below 150 Naira (0.39 USD), and most ideally, to below 50 Naira (0.13 USD).
Current selling prices at pharmacies are around 1000–2000 Naira (2.6–5.2 USD).
Which means our intervention target is to reduce selling costs by 32.5–97.5%.
How can we do this?
- Purchasing supply in bulk (to reduce unit costs)
- Regulating the selling cost (there’s no current regulation at pharmacies)
- Cost-sharing and cross-subsidization models (using donations from a profitable business)
We’re placing the most attention on the first two strategies.
Physical Accessibility
Many of the areas that need this intervention are very rural and remote. Currently, misoprostol for PPH requires a prescription to purchase from a pharmacy.
Pharmacies can be a >12h walk away. Not only is that far, but that’s a day where women can’t work, and where there is no one to take care of their children. All to buy a drug they can’t afford.
It’s our priority to bring misoprostol into the local community/village. There are two steps to this process:
- Having procurement sites locally. Through primary healthcare centres (PHCs) and patent medical vendors (PPMVs).
- TBAs storing a minimum (and maximum) stock to distribute to women after their birth.

Let’s dig into these distribution sites in more depth.
2.1: Procurement Sites
2.1.1: Primary Healthcare Centres (PHCs)
Primary healthcare centres are local “hospitals.” Some of them have a physician; however, most are run by nurses or community health workers. Often, PHCs lack resources like misoprostol. In the case of an emergency, they may not have the means to help the patient.
By using PHCs as a procurement site we can hit two birds with one stone. We stock the health centre with supplies in case of an emergency and they become a place where certified TBAs can purchase their supply at a low price.
Note: the PHCs won’t be selling the drug to the TBAs. We will own the drug and use their site as a storage site. However, we may provide them with a stipend or discount on the supply they purchase. This is to reduce the amount of profit margins required throughout the distribution chain, which makes the drug more affordable for the women.
2.1.2: Proprietary Patent Medical Vendors (PPMVs )
Proprietary patent medical vendors have a license to sell drugs on the approved patent medical list (APML). They aren’t actual pharmacists. However, they’re much more accessible in the communities compared to pharmacies (because they’re located in rural villages).
In Jigawa State there are 5.142M people with 27 local government areas (LGAs). Each LGA has approximately 180,000 inhabitants and 27 PPMVs [3]. In comparison, we could only locate three pharmacies in the state, which is 0.11/ LGA [4].
And, Most of the PPMVs likely aren’t selling misoprostol for PPH. In a study of 600 PPMVs across Abuja and Lagos in Nigeria, 4% had stocked misoprostol in the past, and 3% currently had it in stock. 0% mentioned that it could be used for PPH treatment. (Note as well that this study took place in two large cities. Since we’re working with rural PPMVs, we estimate that these figures are even lower… other than the 0% one, it doesn’t get much lower ;).
Profits from drug sales incentivize PPMVs. This would make the drug more expensive for the end-user because both TBAs and PPMVs will make a (slight) profit. In comparison to just TBAs OR PHCs making a profit.
We’ll select participating PHCs and PPMVs based on proximity to TBAs and input from key local stakeholders [5].
2.2: TBA Storage
Once trained, TBAs will go to their local PPMV/PHC to purchase some misoprostol supply.
You might be wondering: why don’t TBAs just become the procurement centre, why do we need PPMVs/PHCs.
There are two important considerations here: infrastructure and trust.
Infrastructure
Misoprostol needs to be stored at 25°C. It doesn’t need refrigeration. But it does need some cooling given that temperatures in Dutse, Jigawa reach beyond 37°C frequently.
PPMVs store medication like Zinc, which must be kept at about 20° C so it is highly likely they already have the means to store misoprostol safely. We still need to confirm that PHCs have the infrastructure [6].
Trust
Misoprostol is a controversial drug because it can also be used for abortion if a woman takes it before delivery. Right now, misoprostol is a controlled drug.
TBAs can’t read or write. They won’t be trusted with abundant supplies of this product. With small quantities, we can tightly monitor the usage. We need to crawl before we can run.
Storage Details
Each TBA will have a minimum stock of the drug in case of an emergency. This stock has enough misoprostol for 2 women. The dosage is 3–4 misoprostol tablets/women, so assuming the maximum amount is needed, the minimum stock should be 8 tablets.
When replenishing the stock, the TBAs will also have a maximum they can purchase. We are still figuring out an appropriate figure here. Average deliveries/TBA/year is 72. We still have to decide on a maximum purchase quantity.
For example, with this average of 72/year, that’s 6 deliveries/month (not considering seasonal patterns). We could make the maximum purchase quantity/month 48 tablets. This is enough misoprostol for 8 women.
The TBAs hold on to the stock until the woman gives birth. This is to ensure that no one abuses the drug (say, for abortion) before the birth.
TBAs can charge for the misoprostol whenever, but it will likely be part of the delivery cost the woman pays after she has her baby. The total amount they can charge will be regulated.
The TBAs will also create a prescription for each woman she sells to. If she is illiterate, sometimes she will have a literate helper. Otherwise, there we will create a way to easily create prescriptions without literacy. These prescriptions can double as consent forms for data collection.
TBAs sell misoprostol to women. It can be added to the fees they charge to deliver their babies. Every woman can take misoprostol because it can be used as a preventative drug for PPH.
These activities (procurement, TBA storage) work together to lower the barriers to access misoprostol.
3: Monitoring to Ensure Ethical Usage
Under this monitoring section, I will cover:
- Ethical Considerations
- Data Collection at Procurement
- Prescriptions
- Post-Misoprostol Follow-Up
- De-Certification
3.1: Ethical Considerations
The main ethical consideration is ensuring that misoprostol is used only for its intended purposes (PPH).
We need to respect the religious opinions in the areas we operate in. Because misoprostol can be used (and is more commonly used) as an abortion drug, it has a bad perception in Northern Nigeria where abortion is stigmatized.
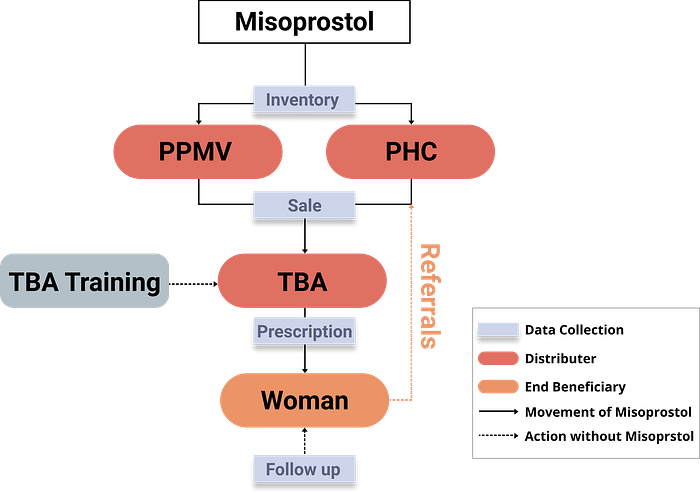
To ensure intended use, we’ve set up an end-to-end data collection system to track misoprostol’s usage. All stakeholders will be aware of this system, including the government.
All data collection spots are in blue.
A secondary consideration is data collection privacy. We will obey Nigeria’s federal health data collection and privacy policies and take necessary precautions.
The rest of this section will be focused on the framework we’re approaching the end-to-end data collection system with because the rest is just legal jargon.
3.2: Data Collection at Procurement
There are two data collection inputs here:
- Inventory Information
- TBA selling information
The main supply of misoprostol can be stored at either PPMVs or PHCs. We are purchasing the supply through a distributor with a wide supply chain in the country.
Each time a new shipment comes into a procurement location, that inventory will be tracked and mapped to the specific procurement centre (either PPMV or PHC).
Once a certified TBA comes to collect their supply, the secretary or storekeeper records selling data.
This is data about:
- Who the TBA [purchaser] is
- Purchase quantity
- Date of purchase
- Location of purchase
3.3: Prescriptions
Time to get creative.
Misoprostol is a controlled drug, so we need to carefully trace each user (while obeying data collection laws).
This is currently done through prescriptions. But TBAs can’t write prescriptions (both legally and literally).
We need a way to track each person purchasing misoprostol while overcoming these two barriers:
- The medical community doesn’t trust TBAs to write prescriptions
- TBAs are illiterate and can’t write prescriptions
3.3.1: Giving TBAs Power to Write Prescriptions [7]
After completing their training certification, TBAs know about using misoprostol for PPH. They’ll only have the ability to prescribe misoprostol.
3.3.2: A medical board will selectively review and oversee the TBAs.
This board can consist of anyone in Nigeria with the power to prescribe misoprostol.
Keeping the prescription scope tight, and having an advisory system helps ensure prescriptions are created safely.
3.3.3: Making Prescriptions Simple
Because TBAs only can prescribe misoprostol under this model, all the medical information is constant. 3–4 tablets of misoprostol intended for PPH prevention/treatment. The only variable is the mother (patient).
From the mother, we would want to know:
- Her name
- Her village and address
- Any contact information
- Her fingerprint or signature (for data-collection consent purposes)
- ** A family member’s contact (this is a nice-to-have)
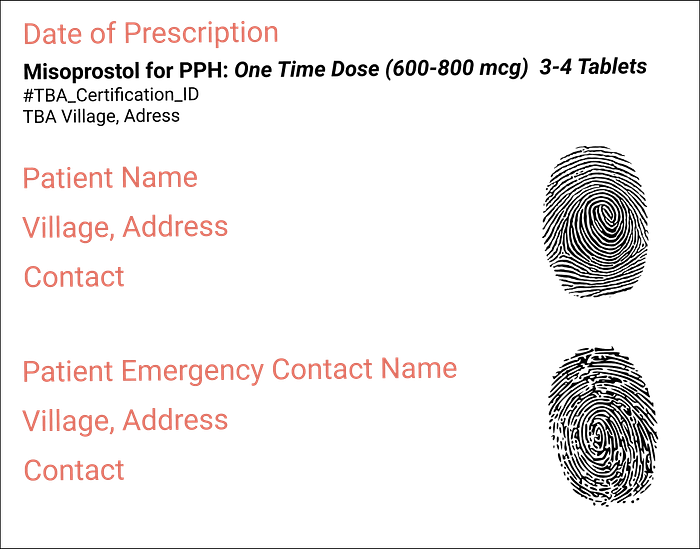
Example prescription
All the pink parts of the prescription is the variable info we’d like to capture. The fingerprints could be replaced with signatures.
What if a TBA can’t write?
We still haven’t finalized the prescription protocol, but this is something we need to design for. We could look at using voice recordings, for example. Or, leveraging the medical advisory board to help transcribe the prescription (through a phone call). Sometimes, TBAs have literate helpers who could also transcribe.
We’ll need to work with the Ministry of Health to create a protocol that makes sense given the resources on-ground.
When a TBA creates a prescription, she still holds onto the drug until the drug needs to be administered — it will be administered by her or a staff at a certified PHC.
3.4: Post-Misoprostol Follow-Up
After the use of misoprostol, we’ll collect some data about the experience. Specifically:
- The dose used for each woman. This can be updated on the prescription. The updated prescription can be submitted to the medical advisory board at this point.
- Recording any adverse effects, including death. Note: Misoprostol doesn’t cause death, but there are still other aspects of maternal mortality that this intervention doesn’t overcome, like infections.
- We’ll have external data collectors randomly review cases without any adverse effects. They will conduct post-misoprostol interviews to understand women’s experiences.
- We’ll have external data collectors review all cases with adverse effects.
3.5: De-Certification
If, at any point during the intervention someone is disobeying the protocol, they may be de-certified and excluded from this intervention.
This applies to both TBAs and PHCs/PPMVs.
4: Referrals to Health Centres
TBAs are the most popular way to give birth in Northern Nigeria.
But they lack the qualifications and resources to deal with many adverse effects. We want to decrease the delay in seeking care and reaching care at a facility when a TBA does not have the skills to save the mother.
Hospital and PHC referrals add a new layer of complexity. While this is extremely important to decrease maternal mortality and strengthen the health system, we have to keep the project scope tight.
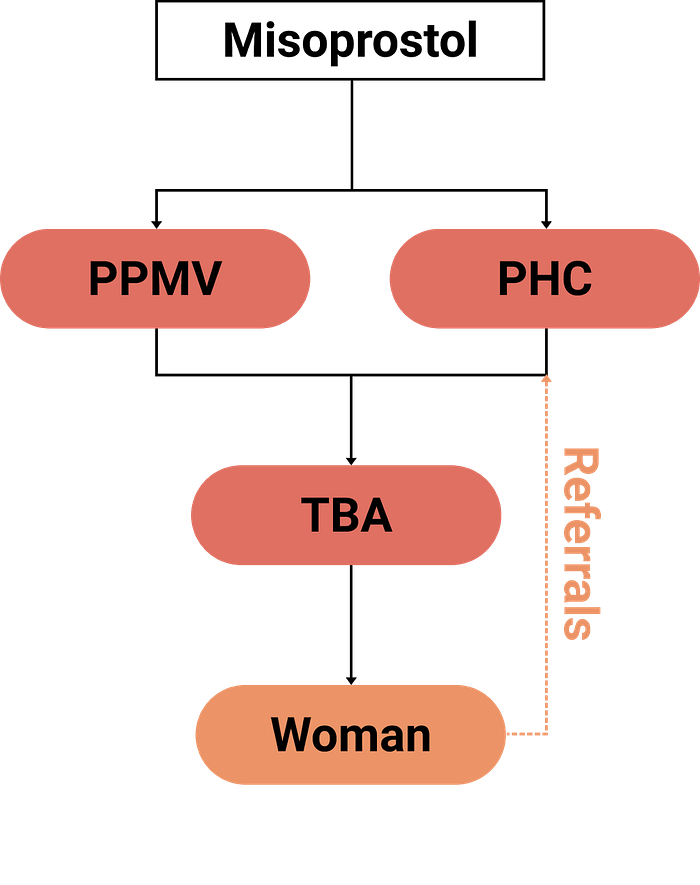
Our program development may not be building the referral infrastructure, but we are certainly open to leveraging existing initiatives/support. Here’s what the updated flow chart would look like.
In terms of hospital referrals, there are 3 things we need to consider:
- Conducting a Facility Needs Assessment
- Physical Transport Issues
- Consent Issues
4.1: Conducting a Facility Needs Assessment
“You should clean the house before inviting people in.” — my mom.
But seriously, we need to ensure the PHCs are functional. If they’re not, there’s no point in sending emergency patients there. To do this, we are collaborating with the ministry of health’s primary healthcare centre division to analyze existing data.
4.2: Physical Transport Issues
OK, if the PHCs are fit for emergency patients, the patients need to get there. In remote, rural areas, this can be a huge challenge, especially since there’s often no roads. A project in Adamawa State, Nigeria, built an emergency transport scheme to help increase access to emergency maternal care — so we know it’s not impossible.
4.3: Consent Issues
Culturally, many women need permission to leave their homes. This might be from her husband or their house head (ex., the grandfather). This can slow down the process of reaching care at the PHCs because of the household bureaucracy.
To overcome this, there may need to be ways to get consent for emergency transport before the delivery starts.
Hospital referrals are complicated. They would be crucial for strengthening the health system, but they are also a massive undertaking.
5: Community Engagement
System strengthening starts from the ground-up.
We can have all the supplies in the world, but if the community doesn’t want to use the intervention, no one’s life can be saved.
One of the most common advice/feedback we get from experts is to get buy-in from important stakeholders — specifically religious and traditional leaders.
As we transition from model development to implementation, community engagement and feedback needs to become the top priority. Our goal is to create a sustainable initiative, not an initiative run by our team. We want our team to become “useless” in the operations as soon as possible. We help supply the skeleton, the community builds the flesh.
This section is less detailed because we’re just transitioning to implementation.
Framework Recap: Distributing Misoprostol
- Upskilling TBAs
- Supplying the Misoprostol
- Monitoring to Ensure Ethical Usage
- Referrals to Health Centres
- Community Engagement
Overall Model
Overall Model
Pre-Pilot Assessments and Activities
Before we start deploying a pilot, there are some activities we still need to do:
General:
- Selecting the LGA(s): using current data + more obtained from the ministry of health
Training:
- Newborn health training materials: as requested from the ministry of health, they’d like to have neonatal training in the curriculum.
- TBA focus group to understand their comfort and concerns with the intervention.
Procurement:
- Pricing assessment: from the perspective of TBAs and women
- Choosing procurement centres: specifically which PHCs and PPMVs to use
Monitoring:
- TBA focus group: on Digital literacy. Used to build data-collection infrastructure
Referrals:
- Needs assessment for PHC materials
- Needs assessment for transport to PHCs
Community Engagement:
- Getting buy-in from LGA leaders and traditional + religious leaders in selected LGA.
Special thanks to Madhav Malhorta, Alishba Imran, Adam Majmudar, Kiran Mak, Ruhani Walia and Shagun Maheshwari for reviewing drafts of this article.
Footnotes:
[1] total MM = 303,000, NG = 58,000 from https://ourworldindata.org/maternal-mortality
However, given that many cases occur in rural, remote areas, it’s highly likely that these cases are severely underreported and both of these figures are higher.
[2] A combination of literature + our on-ground contacts have helped to highlight the importance of incentives beyond money. For an example study, see: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5777388/
[3] There are 14.9 PPMVs / 100,000 people. Almost 50% of the 770 shops are in rural areas.
[4] There are likely more pharmacies that don’t have a good digital presence. However, our local contacts emphasize that PPMVs are more accessible and affordable than pharmacies anyway.
[5] Several parts of the exact details of the model depend on regulations and approvals. We’ll need to seek medical and ethical clearance from the Federal and State government. This process will very likely alter the exact details of distribution.
[6] The state of all medical facilities vary in Jigawa. We will need to evaluate each facility before entering the pilot. Currently, this data is unavailable to us.
[7] Giving TBAs prescription-writing power is a controversial topic. The last thing we want is for them to purchase large supplies of inexpensive misoprostol to resell on the black market. This is still an aspect of the framework that we’re revisiting and is subject to change.
